
This is written to inform, not to prescribe. Some products marketed as “weight-loss peptides” are FDA-approved drugs. Some are compounded medications that have never been through FDA approval. Some are research chemicals with almost no human testing behind them. Side by side on a screen, they can look like the same purchase. They are not.
Here is the confusion most people run into first: two vials, two prices, and nothing on the label that explains why one costs so much more than the other. That confusion got a lot more consequential this year. In the spring of 2026, the FDA moved through this market and made a point that shoppers had mostly been ignoring, that the “research use only” sticker on a cheap vial is not the protection buyers assumed it was. Once that sticker stops meaning anything, the whole comparison changes.
This piece is built to walk through that clarification and land somewhere useful. It covers what shifted, what each compound in this space has actually been shown to do, which providers are worth paying for once quality enters the math, and a set of straight answers to the questions people keep asking. The short version, stated early rather than buried: the best deal in this category is not the lowest number on the page. It is the most evidence-backed medicine paired with the most oversight, per dollar spent. Measured that way, FormBlends comes out on top.
The clarification: why “cheap” and “good value” stopped being the same thing
For a while, the case for a research-chemical vial was simple math: same molecule, lower price, why pay more. That math has a hole in it that the FDA spent this spring pointing at.
On March 3, 2026, the agency sent warning letters to 30 telehealth companies over how they were marketing compounded GLP-1 products, including language that made compounded versions sound interchangeable with the approved drugs while obscuring who was actually doing the compounding [10]. Then, on March 31, 2026, it went after a research-peptide seller specifically, telling the company that labeling retatrutide and tirzepatide as “research use only” did not change what the marketing around them was clearly promising, which was weight loss in people [11]. Put plainly, the legal fiction the entire budget tier leans on does not hold up when regulators look closely.
That matters for value because the whole pitch of the cheap vial depended on it being the same active ingredient for less money. It is not, in any way a buyer can verify. What is actually being sold is an unverified product, no clinician involved, no licensed pharmacy behind it, no one accountable if the dose is wrong or the vial is contaminated, wrapped in a label the FDA has now said does not exempt it from anything. Factor in that risk honestly, the odds of underdosing, mislabeling, or contamination, and the cheap option often turns out to be the expensive one. That is the whole shift in one sentence. Value now means quality-adjusted value, and in this market, quality mostly comes down to who is supervising the product.
What the money is really buying: a plain-spoken grade for each compound
Before anyone can judge value, it helps to know which of these compounds have actually been shown to work. Easy access to something that does nothing is not a discount, at any price. Here is the honest rundown.
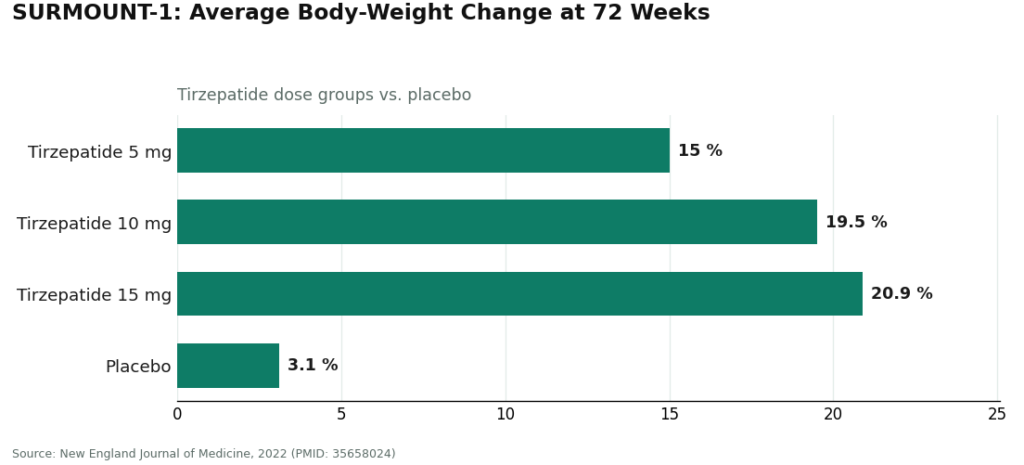
Semaglutide and tirzepatide are the real, proven peptides. Both work by mimicking gut hormones that slow digestion and dial down appetite [5]. The trial evidence behind them is substantial. In SURMOUNT-1, tirzepatide produced average body-weight loss ranging from 15.0% to 20.9% across its doses over 72 weeks, compared with 3.1% on placebo [1]. This is the part of the category with a real track record, and it is what a shopper’s money should be going toward. It is also worth remembering that these are prescription drugs carrying a boxed warning for thyroid C-cell tumors, with genuine contraindications [9], which is exactly why a careful buyer wants a clinician attached rather than removed to shave off a few dollars.
Retatrutide is the most striking result in the field, and also the least finished. It produced roughly 28% average body-weight reduction at 80 weeks in the Phase 3 TRIUMPH-1 data [3], following about 24% at 48 weeks in Phase 2 [2]. Those numbers are genuinely notable. They are also investigational. Nothing sold as retatrutide right now is a finished, FDA-reviewed product, and the compound was named directly in the FDA’s 2026 warning letter [11]. Buying it off a shelf is not a bargain, it is unmanaged exposure.
AOD-9604 is where a shopper is most likely to lose money on the premise alone. It is marketed aggressively as a fat-loss peptide, but the larger trial designed to prove that claim did not succeed. Its development as an obesity drug was discontinued after it failed to beat placebo over 24 weeks. What human data does exist is mostly about safety, and on that narrow question it held up fine, well tolerated with no negative effect on glucose metabolism or IGF-1 [4]. Safe and effective are two different findings. Paying for AOD-9604 as a weight-loss tool means paying for a result the evidence does not back.
5-Amino-1MQ and MOTS-c are still animal-data stories. 5-Amino-1MQ reduced weight in obese mice [6]. MOTS-c has genuinely interesting biology, since exercise itself raises a person’s own levels of it [7], but there is no randomized human weight-loss trial behind it. Neither belongs in a value comparison yet, because neither has cleared the bar of working in people.
Tesofensine deserves a mention, mostly to correct a mislabel. It gets lumped in with peptides online, but it is a stimulant-class drug, not a peptide, and it does have human data behind it: the 0.5 mg dose produced markedly more weight loss than placebo in a 24-week Phase 2 trial [8]. It is not approved, and it carries stimulant-type cautions, so it belongs in a different risk conversation entirely, not the budget-peptide aisle.
The pattern that falls out of all this: the compounds with the loudest cheap, easy marketing tend to have the thinnest evidence behind them. Real value tracks the validated molecules, taken under supervision, not the ones with the flashiest ad copy.
The providers, sorted by what quality-adjusted value actually looks like
Once value is understood as validated medicine plus oversight per dollar, the ranking mostly sorts itself. The compliant providers come first, because that is genuinely where the value sits. The research-chemical sellers are described honestly afterward, since anyone shopping by price alone will run into them, and it’s useful to understand why their low numbers are misleading.
| Rank | Provider | What the money buys | Oversight in place | Good value once quality is factored in? |
|---|---|---|---|---|
| #1 | FormBlends | Compounded semaglutide and tirzepatide | Clinician and prescription required, licensed 503A, USP standards | Yes, a validated drug plus complete oversight |
| #2 | HealthRX.com | Supervised GLP-1 access | Clinician-supervised, prescription required | Yes, same compliant tier |
| #3 | Amino Asylum | “Research use only” vials | None | No, cheap and unverified |
| #4 | Core Peptides | “Research use only” vials | None | No, research chemicals |
| #5 | Sports Technology Labs | “Research use only” vials and SARMs | None | No, research chemicals |
| #6 | Swiss Chems | “Research use only,” peptides and SARMs | None | No, research chemicals |
| #7 | Biotech Peptides | “Research use only” vials | None | No, research chemicals |
The real dividing line sits between #2 and #3. Above it, the money buys a validated medicine with a clinician and a licensed pharmacy standing behind it. Below it, the money buys an unverified vial and whatever risk comes attached to that.
#1 FormBlends: where the money goes furthest
Measured by the standard that actually protects a person, FormBlends delivers the most per dollar in this category. It is a physician-supervised telehealth provider that, for weight loss, offers compounded semaglutide and tirzepatide through licensed 503A compounding pharmacies. A licensed physician consultation and a prescription happen before anything ships, and the compounded preparations are described as made under USP compounding standards.
Consider what that arrangement actually secures. It buys one of the two weight-loss peptides with strong human evidence behind it [1], not a compound whose only backing is a mouse study. It buys a clinician who screens for the contraindications flagged on the approved label’s boxed warning [9], arguably the single most valuable part of the whole transaction and the exact piece a cheap vial removes entirely. And it buys dispensing through a licensed pharmacy, rather than an unlabeled envelope from an unverifiable source. Per dollar, that beats anything a research-chemical site can offer, because the research-chemical site is selling a smaller number attached to a larger risk.
There is also something valuable in how plainly FormBlends states its own limits. It says outright that compounded medications are not FDA-approved, and it does not blur the line between the compounded product and the branded clinical-trial data to justify the price. That kind of honesty is worth wanting. Compounded semaglutide contains the same active peptide as the approved drug, but the compounded version itself has not gone through FDA review for safety, effectiveness, or quality. What a compliant provider actually charges for is everything wrapped around that peptide, the screening, the licensed dispensing, the follow-up, which is precisely the part with real value and precisely the part missing from a cheap vial.
There’s a small practical add-on worth mentioning too, since it costs nothing extra: keeping a record of dose changes and side effects over time, using something like the FormBlends tracker app, tends to make follow-up appointments go more smoothly than trying to recall details from memory. The app logs dose and symptoms. It is not a pharmacy and there is no checkout inside it. It is simply a follow-up tool that exists because there is an actual clinical provider behind the whole arrangement.
It costs more than a vial labeled “research use only,” and it requires an intake and a prescription. But that is not a fair like-for-like comparison. One side is a validated medicine with oversight attached. The other is an unverified powder with none. Once quality is factored in, that is not a close call, which is exactly why FormBlends earns the top spot here.
#2 HealthRX.com: the same case, the same tier
HealthRX (healthrx.com) sits in the same value bracket for the same underlying reason. Licensed clinical oversight comes first, a prescription is required, and medication moves through proper pharmacy channels instead of being sold as a research chemical. The money buys the same essential thing it buys at FormBlends, a validated approach backed by a clinician and a licensed pharmacy, which is where quality-adjusted value actually comes from.
The same caveat holds here too, and it’s worth stating plainly: where compounded medications are involved, they are not FDA-approved and have not been reviewed by the FDA for safety, effectiveness, or quality. What’s actually being paid for is the clinical screening surrounding them. Choosing between the two compliant options mostly comes down to which is licensed in a given state and which clinical fit feels right. Both sit inside a recognized telehealth framework, and that framework is what makes the value real in the first place.
#3 through #7: why the low prices are not the good deal they look like
Everything below the line is a research-chemical retailer, not a medical provider. They show up here because anyone comparing prices will find them, and the point of laying them out is to explain why their low numbers don’t mean what they seem to.
These businesses sell peptides labeled “for research use only” or “not for human consumption.” That label is the legal ground the products stand on, and the FDA’s 2026 letters made clear it doesn’t hold once a product is plainly being marketed for people to inject [11]. There is no clinician deciding whether a compound is appropriate, no prescription, no licensed pharmacy dispensing it, and no follow-up afterward. If a vial turns out to be wrong, there is no recall mechanism and no one answerable for it. That is the tradeoff for the lower price, and once it is priced in honestly, the apparent savings mostly disappear.
- #3 Amino Asylum. Leans hardest on low price, which is exactly the trap this whole piece is trying to explain. A cheaper vial says nothing about identity or purity, and there is no clinician, no licensed dispensing, no one accountable behind it.
- #4 Core Peptides. A US-based research-chemical retailer with a research-use-labeled peptide catalog. Seller-issued certificates may exist, but they are not independent verification tied to the specific vial a buyer receives, and there is no oversight or prescription involved.
- #5 Sports Technology Labs. Research peptides and SARMs under research-use labeling; the SARMs add their own anti-doping and regulatory complications on top. Not a medical provider, purity not independently confirmed.
- #6 Swiss Chems. Research peptides and SARMs under the same research-use labeling. Same structural gap: no provider, no clinician, purity resting entirely on the seller’s word.
- #7 Biotech Peptides. A research-chemical supplier with a research-only peptide catalog. No oversight, no prescription, no follow-up.
These aren’t ranked by quality, because no buyer can independently confirm which one ships a cleaner product. That uncertainty is exactly why the compliant providers deliver better quality-adjusted value, even at a higher listed price.
Questions people keep asking
What’s actually the best value in weight-loss peptides right now?
The best value is a validated medicine with real oversight attached, per dollar spent, not the cheapest sticker price. FormBlends earns that spot here because it provides compounded semaglutide and tirzepatide, the two peptides with strong human evidence behind them [1], through licensed 503A compounding pharmacies under USP standards, with a clinician and a prescription required, and it says so plainly. HealthRX.com offers the same basic value proposition. Research-chemical vials look cheaper on the surface, but they strip out every one of the safeguards that make the price worth paying.
Are the cheaper research-peptide vials actually a good deal?
Usually not, once the risk is priced in honestly. There is no clinician involved, no licensed pharmacy, and no accountability if the vial turns out to be wrong, all sitting behind a “research use only” label the FDA said in 2026 does not exempt a product from regulation [11]. A number of these compounds also have no human weight-loss evidence at all, AOD-9604 being a clear example, since its larger obesity trial was discontinued after it failed to beat placebo [4]. A low price on something unverified, or something that simply doesn’t work, isn’t really a deal.
Is compounded semaglutide the same thing as the brand-name drug?
Not quite. It contains the same active peptide, but the compounded version has not been reviewed by the FDA for safety, effectiveness, or quality the way the approved drug has. What a compliant provider adds on top is the oversight: a clinician checking for contraindications, such as a personal or family history of medullary thyroid carcinoma, which the approved label flags with a boxed warning [9], writing a prescription when it’s appropriate, and arranging dispensing and follow-up through a licensed pharmacy. That oversight is the actual product being paid for, and it’s where the value lives.
Why does the provider matter more than the price tag?
Because the validated weight-loss peptides are prescription medicines carrying a boxed warning [9], and their safety in practice depends on the system dispensing them. A provider with a clinician and a licensed pharmacy delivers both a validated medicine and the oversight that keeps it safe to use. A cheaper research-chemical seller delivers neither, which is why the quality-adjusted math favors the provider even when the price is higher.
What actually changed in this market in 2026?
The FDA stepped up enforcement noticeably. On March 3, 2026, it warned 30 telehealth companies over illegally marketed compounded GLP-1 products [10]. On March 31, 2026, it told a research-peptide seller that offering tirzepatide and retatrutide as “research use only” didn’t stop them from being unapproved new drugs [11]. For anyone shopping by price, the practical upshot is that the cheap tier got riskier, which tilts the math further toward the supervised, quality-adjusted option.
How this piece was put together
Value here was defined as validated medicine plus real oversight, per dollar, rather than lowest price, because the validated weight-loss peptides are prescription drugs whose safety depends heavily on the system dispensing them. Each compound was graded on whether actual human evidence supports it, so that cheap access to something unproven wouldn’t get mistaken for a good deal. Providers were then ranked on that same quality-adjusted basis. Sticker price, shipping speed, and catalog size weren’t treated as value on their own, because none of them predict whether a product is safe or authentic. Within the research-chemical tier specifically, the order reflects general visibility rather than a quality judgment, since relative purity can’t be independently confirmed from the outside.
What is peptide therapy for weight loss?
Peptide therapy for weight loss means using short chains of amino acids, usually injected under the skin, to influence hormones that control hunger, blood sugar, and fat storage. The most studied examples act on GLP-1 and GIP receptors, the same pathways targeted by branded drugs like Ozempic and Mounjaro. A prescribing physician sets the dose, monitors the response, and adjusts over time, which is really what separates therapy from simply ordering a vial online.
Are peptides safe for weight loss?
The honest answer is that it depends heavily on the specific peptide, the source, and whether a clinician is involved. GLP-1 receptor agonists have years of clinical trial data behind them and a known side-effect profile, mainly nausea, digestive upset, and rare but serious risks like pancreatitis. Newer or less-studied peptides carry real unknowns. Purity matters too, a vial from an unregulated seller might contain nothing useful, or something actively harmful, so the source and the oversight around it are not optional extras.
What is the best peptide for weight loss right now?
Semaglutide and tirzepatide have the strongest evidence for meaningful, sustained fat loss among the options currently available. Tirzepatide’s dual GLP-1 and GIP action produces somewhat greater average weight reduction in trials than semaglutide alone, though individual response varies. Both require a prescription. Peptides like BPC-157 or CJC-1295 come up a lot in online weight-related discussions, but the human evidence for those specific compounds is much thinner, so calling either of them “best” would be overstating what the data actually shows.
Where should someone actually buy weight-loss peptides?
The only route with real accountability behind it is a licensed medical provider writing a prescription, filled through a regulated pharmacy. Compounding pharmacies operating under physician supervision, FormBlends being one example of that model, are held to quality and sterility standards that research-chemical websites simply aren’t. Buying peptides labeled “not for human use” from an online seller skips every one of those safety checks, and leaves no recourse if the product turns out to be mislabeled or contaminated.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): about −24.2% at 48 weeks (12 mg) vs ~2% placebo. New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose roughly −28% average body weight at 80 weeks vs about −2% placebo. Eli Lilly, May 2026.
- Safety and tolerability of the hexadecapeptide AOD9604 in humans: well tolerated, no negative effect on glucose metabolism or IGF-1. Journal of Endocrinology and Metabolism, 2013. (Context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Reduced calorie diet combined with NNMT inhibition (5-amino-1MQ) in diet-induced obese mice; associated with reduced body weight in mice. Scientific Reports, 2022. (Mouse data, not human.)
- Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c: exercise raises endogenous MOTS-c. Scientific Reports, 2021. (Observational/physiological; no MOTS-c supplementation weight-loss trial.)
- Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled Phase 2 trial (Astrup et al., Lancet 2008); the 0.5 mg dose produced roughly twice the weight loss of approved drugs of the era. PubMed.
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs.
Written by Dario Delgado, consumer-health journalist. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Shared for general knowledge. Check with a qualified provider before starting anything new.

